One of the lessons that the COVID-19 pandemic has taught us is that the advent of an unexpected medical danger can have ripple effects that go well-beyond just the specific health matters at hand.
One that has been well-covered in the news is how the precautions most people are taking to avoid contracting the coronavirus are driving flu cases down to levels never before seen. This chart pretty much says it all: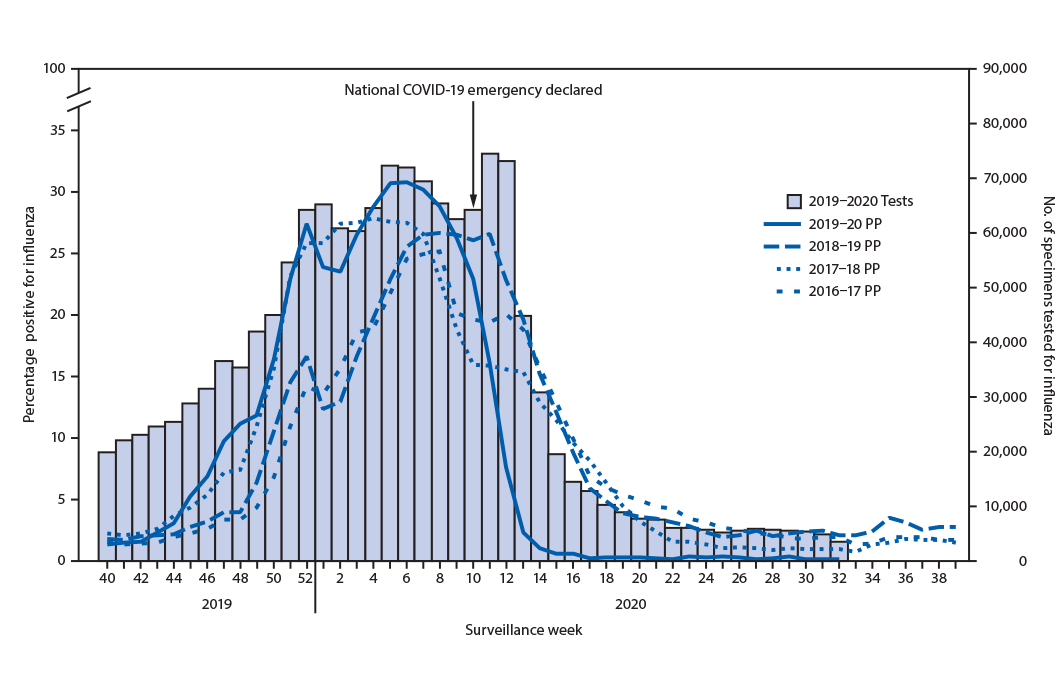 But as it turns out, there are some other, perhaps more unanticipated consequences — ones that have positive and negative aspects.
But as it turns out, there are some other, perhaps more unanticipated consequences — ones that have positive and negative aspects.
 We’re reminded of this in the form of several newly published reports. One report comes from Altria, the largest U.S. producer of tobacco products. According to Altria, the onset of the COVID-19 pandemic appears to be responsible — at least in part — to halting a decades-long steady decline in cigarette usage among Americans.
We’re reminded of this in the form of several newly published reports. One report comes from Altria, the largest U.S. producer of tobacco products. According to Altria, the onset of the COVID-19 pandemic appears to be responsible — at least in part — to halting a decades-long steady decline in cigarette usage among Americans.
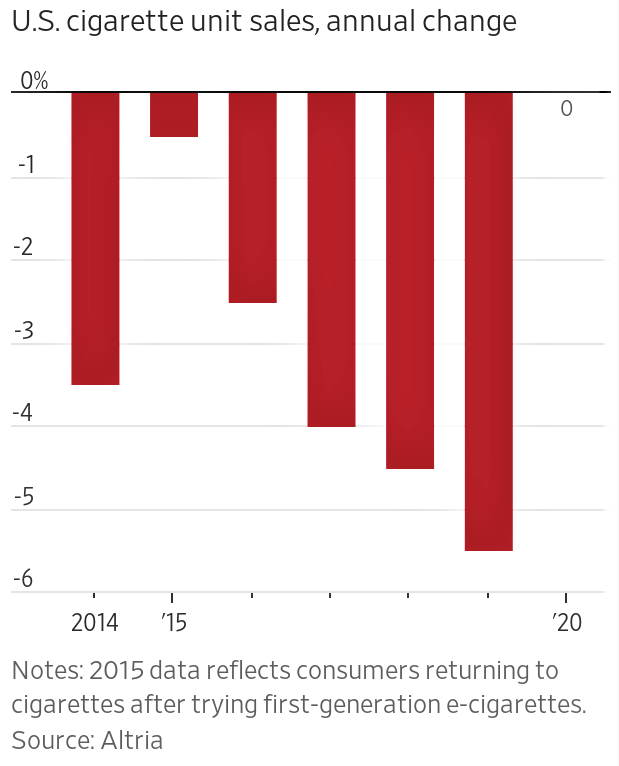
While the trend hasn’t actually gone in reverse, Altria does report that in 2020, the cigarette industry’s unit sales in the U.S. were flat as compared to 2019.
That’s a big shift from the 5.5% annual decline in usage that was observed between 2018 and 2019.
 As for the reasons behind such a sudden shift in consumer behavior, the Altria report touches on several probable factors, including:
As for the reasons behind such a sudden shift in consumer behavior, the Altria report touches on several probable factors, including:
- People had more opportunities to smoke because of spending more time at home rather than the office.
- More disposable income available for smokes because of less money being spent on commuting, travel and entertainment expenses.
- The heretofore-robust growth of substitute products (e-cigarettes) was reversed in response to reports about unexplained lung illnesses among e-cigarette users, the ban on flavored vaping products, plus increased taxes on e-cigarette products.
- A more acute sense of personal stress and anxiety in the wake of the coronavirus pandemic.
The newest trends in cigarette usage can’t be good for seeing a return to the decline in death rates that are tied to smoking. Unfortunately, those rates remain high: The effects of smoking account for more than 480,000 deaths in the United States each year.
On the other hand, there are positive ripple effects related to the coronavirus pandemic, too. As it turns out, the medical innovations that have been part of the worldwide response to the pandemic are delivering parallel positive benefits in the broader war on cancer.
One piece of evidence is the success of newly developed mRNA vaccines for combating the COVID-19 virus. Those same vaccines are now being repurposed to battle various forms of cancerous tumors.
Naturally, any such development on the cancer treatment front won’t be a quick “silver bullet” solution in the decades-long battle to defeat cancer. But a report released in January 2021 by the American Cancer Society points to the promising success that such new initiatives are having.
 The key stats are telling: American cancer death rates have dropped steadily since 1991 – with an overall decrease of ~31% in the death rate through 2018 that was capped by a one-year decline of ~2.5% observed in 2017-18 alone.
The key stats are telling: American cancer death rates have dropped steadily since 1991 – with an overall decrease of ~31% in the death rate through 2018 that was capped by a one-year decline of ~2.5% observed in 2017-18 alone.
The ACS report summarizes:
“An estimated 3.2 million cancer deaths have been averted from 1991 through 2018 due to reductions in smoking, earlier [cancer] detection, and improvements in treatment, which are reflected in long-term declines in mortality for the four leading cancers: lung, breast, colorectal and prostate.”
Not surprisingly, lung cancer is the biggest driver of the death rate decline. Whereas a dozen years ago the overall survival rate for non-small cell lung cancer was just 34%, in 2015 it was 42% (and it’s higher today).
Looking forward, even as we eagerly anticipated the large-scale rollout of COVID-19 vaccinations which can’t come soon enough, we can also be happy in the hope that the emerging science will deliver a parallel positive impact on cancer treatments – so long as we can convince people not to regress in their smoking habits.
What lifestyle adjustments – positive or negative – have you or people you know made over the past year? Beyond the risks of the coronavirus itself, what other new health challenges have you or they faced in its wake? Please share your perspectives with other readers here.